The opioid epidemic, a devastating public health crisis, has been fueled by a complex interplay of factors, including overprescription of opioid painkillers, aggressive marketing by pharmaceutical companies, and the proliferation of highly addictive synthetic opioids like fentanyl. The initial wave of the epidemic was driven by the widespread availability of prescription opioids, often prescribed for chronic pain despite limited evidence of their long-term efficacy. As regulatory measures tightened access to prescription drugs, many individuals turned to cheaper and more potent illicit alternatives, such as heroin and fentanyl, exacerbating the crisis. Socioeconomic factors, including poverty, unemployment, and lack of access to mental health services, have also played a significant role, as marginalized communities often bear the brunt of the epidemic. Additionally, systemic failures in healthcare, education, and policy have perpetuated the cycle of addiction, making the opioid crisis a multifaceted issue that demands comprehensive and coordinated solutions.
| Characteristics | Values |
|---|---|
| Overprescription of Opioids | In 2021, U.S. healthcare providers wrote 139.3 opioid prescriptions per 100 persons, though rates have declined since 2012 (CDC, 2023). |
| Pharmaceutical Marketing | Aggressive marketing by companies like Purdue Pharma misrepresented addiction risks (e.g., OxyContin lawsuits). |
| Transition to Illicit Drugs | 80% of heroin users reported misusing prescription opioids first (NIH, 2022). Fentanyl-laced drugs now drive 70% of opioid deaths. |
| Economic and Social Factors | High rates of opioid deaths in economically distressed areas (CDC, 2023). Poverty, unemployment, and lack of access to healthcare are key risk factors. |
| Lack of Access to Treatment | Only 1 in 5 people with opioid use disorder (OUD) receive medication-assisted treatment (MAT) due to stigma, cost, and provider shortages (SAMHSA, 2023). |
| Fentanyl Contamination | Fentanyl involved in 84% of opioid-related overdose deaths in 2022 (CDC, 2023). Often mixed with heroin, cocaine, or counterfeit pills. |
| Stigma and Underfunding | Stigma reduces treatment-seeking; federal funding for OUD treatment remains inadequate compared to other chronic diseases (NAM, 2023). |
| Mental Health Comorbidities | 50% of individuals with OUD have co-occurring mental health disorders (NIDA, 2023), often untreated due to fragmented care systems. |
| Racial Disparities | Black individuals are less likely to receive opioids for pain but face higher fentanyl-related death rates due to systemic inequities (CDC, 2023). |
| Policy Gaps | Inconsistent implementation of Prescription Drug Monitoring Programs (PDMPs) and limited naloxone distribution in high-risk areas. |
Explore related products






What You'll Learn
![]()
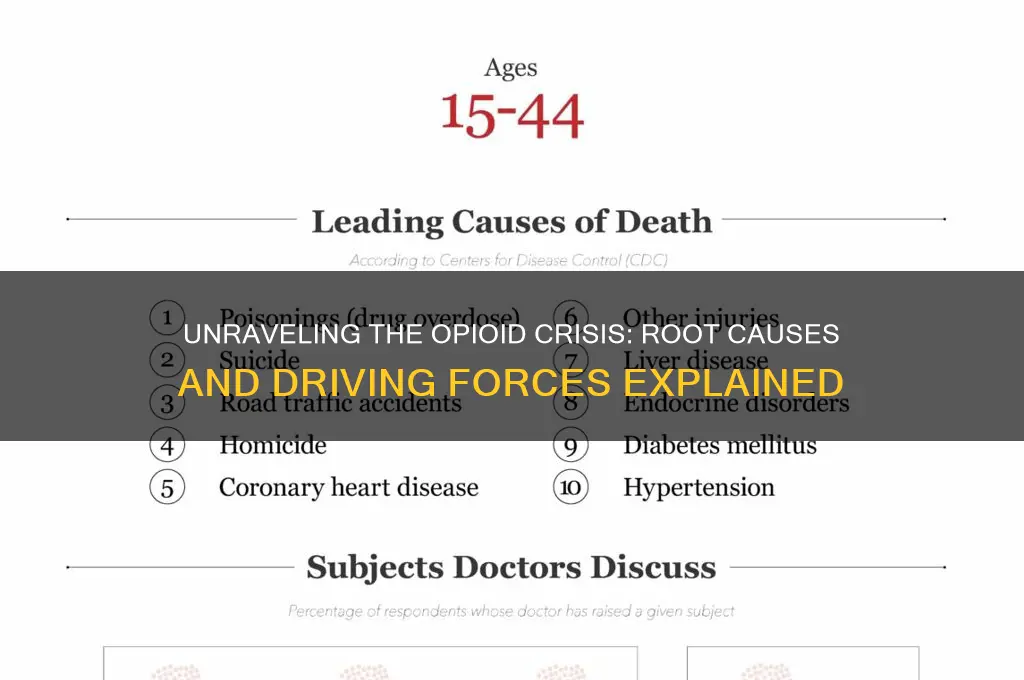
Overprescription of painkillers by healthcare providers
The overprescription of painkillers by healthcare providers has been a significant driver of the opioid epidemic, contributing to widespread addiction, overdose, and death. Data from the Centers for Disease Control and Prevention (CDC) reveals that in 2012, healthcare providers wrote 259 million opioid prescriptions—enough for every adult in the U.S. to have a bottle of pills. This excessive prescribing often stems from a combination of aggressive pharmaceutical marketing, inadequate provider training in pain management, and a cultural expectation for quick relief from pain. For instance, a single dental procedure like wisdom tooth extraction can result in a 30-count prescription of hydrocodone (5 mg per pill), far exceeding the 3-day supply now recommended by the CDC for acute pain.
Consider the mechanics of how overprescription fuels addiction. When opioids are prescribed in high doses or for extended durations, patients develop tolerance and physical dependence. A patient prescribed oxycodone (10 mg, 3 times daily for 30 days) for chronic back pain may find themselves needing higher doses to achieve the same pain relief within weeks. This cycle often leads to misuse, as patients take more pills than prescribed or use them beyond the intended timeframe. Alarmingly, studies show that up to 6% of patients prescribed opioids for chronic pain develop an opioid use disorder within a year. Healthcare providers, often pressured by patient demands or lacking alternatives, inadvertently become gatekeepers to addiction.
To address this issue, providers must adopt evidence-based prescribing practices. For acute pain, such as post-surgical recovery, prescriptions should be limited to 3–5 days, with dosages starting at the lowest effective level (e.g., 5 mg of oxycodone every 6 hours as needed). For chronic pain, opioids should be a last resort, used only after non-opioid therapies (physical therapy, NSAIDs, or antidepressants) have failed. Providers must also utilize prescription drug monitoring programs (PDMPs) to track patient histories and identify potential misuse. For example, a dentist prescribing hydrocodone should check the PDMP to ensure the patient hasn’t received similar prescriptions from other providers recently.
However, shifting prescribing habits requires systemic change. Medical schools and continuing education programs must prioritize pain management training, emphasizing non-opioid alternatives and the risks of overprescribing. Policymakers can enforce stricter prescribing guidelines, as seen in states like New York, which limits opioid prescriptions for acute pain to 7 days. Patients also play a role by advocating for non-opioid treatments and properly disposing of unused medications—a single leftover pill can be a gateway to misuse. By rethinking prescription practices, healthcare providers can break the cycle of overprescription and mitigate their role in the opioid crisis.
Are Indy Fuel Earbuds Waterproof? A Comprehensive Review and Guide
You may want to see also
Explore related products





![]()
Illicit fentanyl flooding the black market
Illicit fentanyl has become the silent assassin of the opioid epidemic, infiltrating drug supplies with deadly precision. This synthetic opioid, up to 100 times more potent than morphine, is often mixed into heroin, cocaine, or pressed into counterfeit pills resembling prescription medications like OxyContin or Xanax. A dose as small as 2 milligrams—equivalent to a few grains of sand—can be fatal, yet dealers and users often remain unaware of its presence. This invisibility transforms every purchase into a game of Russian roulette, driving overdose rates to unprecedented heights.
Consider the mechanics of this crisis: fentanyl’s low production cost and high potency make it a lucrative additive for drug traffickers. A kilogram of fentanyl, costing as little as $5,000 to produce, can generate over $1 million in street sales when mixed into other drugs. This economic incentive fuels its proliferation, particularly in regions where heroin supplies are unstable or expensive. For instance, in the Midwest and Northeast U.S., fentanyl has almost entirely replaced heroin in the illicit market, becoming the primary driver of opioid-related deaths in these areas.
The public health response to this crisis has been reactive rather than proactive. Harm reduction strategies, such as fentanyl test strips, offer users a way to detect the drug’s presence in their supply, but these tools are often illegal in states with restrictive drug paraphernalia laws. Meanwhile, naloxone, the overdose reversal medication, struggles to keep pace with fentanyl’s potency, often requiring multiple doses to revive a victim. Without broader access to these tools and a shift in policy to decriminalize harm reduction efforts, the death toll will continue to rise.
To combat this crisis, a multi-pronged approach is essential. First, law enforcement must target the supply chain, focusing on the illicit labs in China and Mexico that produce fentanyl and the dark web networks that distribute it. Second, healthcare providers should expand access to medication-assisted treatment (MAT), such as buprenorphine and methadone, which reduce cravings and withdrawal symptoms, lowering the demand for street drugs. Finally, public education campaigns must emphasize the dangers of fentanyl, particularly among young adults aged 18–35, who represent the fastest-growing demographic of opioid overdose victims.
In conclusion, illicit fentanyl is not just another drug in the opioid epidemic—it is the accelerant that has turned a public health crisis into a national emergency. Its invisibility, potency, and profitability create a perfect storm of risk, demanding urgent, coordinated action. Without addressing the unique challenges posed by fentanyl, efforts to curb the opioid epidemic will fall short, leaving countless lives at stake.
What Fuel Do Planes Use? Exploring Aviation Fuel Types and Efficiency
You may want to see also
Explore related products





![]()
Lack of access to addiction treatment
The opioid epidemic rages on, claiming lives and devastating communities, yet a critical barrier stands in the way of recovery: access to treatment. Millions of individuals struggling with opioid addiction are denied the very tools they need to break free.
Imagine a fire raging, but the fire hydrants are padlocked. This is the reality for many seeking help for opioid addiction.
The Treatment Desert:
Geography plays a cruel role in this crisis. Rural areas, often hardest hit by the opioid epidemic, are treatment deserts. A 2018 study found that over 60% of rural counties in the US lack a single physician licensed to prescribe buprenorphine, a highly effective medication for opioid use disorder. This means individuals in these areas face hours-long drives, if they have transportation at all, to reach treatment centers. For someone battling addiction, the logistical hurdles can be insurmountable.
Urban areas fare little better. While treatment facilities may exist, they are often overwhelmed, with waitlists stretching for months. This delay can be fatal, as the risk of overdose remains high during this vulnerable period.
Financial Barriers: A Vicious Cycle
Even when treatment is geographically accessible, cost often becomes the next insurmountable obstacle. Many insurance plans offer limited coverage for addiction treatment, leaving individuals with exorbitant out-of-pocket expenses. For those without insurance, the situation is dire. A month of inpatient treatment can cost upwards of $20,000, a sum far beyond the reach of many struggling with addiction, who often face unemployment and financial instability.
Stigma: The Silent Killer
Beyond the tangible barriers of location and cost, stigma casts a long shadow. The pervasive misconception that addiction is a moral failing rather than a chronic disease discourages many from seeking help. Fear of judgment from healthcare providers, employers, and even family members keeps people trapped in a cycle of shame and isolation. This stigma extends to medication-assisted treatment (MAT), with some viewing it as simply replacing one drug with another. In reality, MAT, which combines medications like methadone or buprenorphine with counseling and behavioral therapies, has been proven to significantly improve treatment outcomes and reduce overdose deaths.
Breaking the Chains:
Expanding access to treatment requires a multi-pronged approach. Increasing the number of healthcare providers trained in addiction medicine, particularly in rural areas, is crucial. Telehealth services can bridge the geographical gap, allowing individuals to access counseling and medication management remotely. Insurance reforms are essential to ensure comprehensive coverage for addiction treatment, removing the financial burden that prevents so many from seeking help. Finally, public education campaigns are needed to combat stigma, fostering understanding and compassion for those struggling with addiction.
The opioid epidemic is a complex crisis, but expanding access to treatment is a crucial step towards stemming the tide of devastation. By addressing the barriers of geography, cost, and stigma, we can offer a lifeline to those in need and begin to heal the wounds inflicted by this epidemic.
Understanding Bunker Fuel Production: A Comprehensive Guide to Its Manufacturing Process
You may want to see also
Explore related products






![]()
Pharmaceutical companies' aggressive marketing tactics
Pharmaceutical companies have played a pivotal role in fueling the opioid epidemic through aggressive marketing tactics that prioritize profits over public health. One of the most notorious examples is Purdue Pharma’s campaign for OxyContin, which involved misleading claims about the drug’s safety and efficacy. Sales representatives were trained to downplay addiction risks, falsely asserting that less than 1% of users would become dependent. This misinformation was disseminated to doctors, pharmacists, and patients, leading to widespread overprescription. By 2001, OxyContin prescriptions had surged to 6.2 million annually, a tenfold increase from its launch in 1996, directly contributing to the rise in opioid addiction and overdose deaths.
To understand the scale of this strategy, consider the financial incentives driving these campaigns. Pharmaceutical companies spent billions on marketing opioids, often targeting primary care physicians rather than pain specialists. For instance, Purdue Pharma’s budget for OxyContin promotion exceeded $200 million annually in the early 2000s. Tactics included lavish dinners, all-expenses-paid trips, and speaker fees for doctors who prescribed their drugs. These efforts were so effective that by 2015, 99% of U.S. doctors had received payments from pharmaceutical companies, with opioid manufacturers among the top contributors. Such practices created a culture of overprescription, as physicians were incentivized to prioritize branded medications over patient safety.
A critical analysis of these marketing tactics reveals a systemic failure in regulatory oversight. The FDA approved opioids like OxyContin based on short-term studies, despite lacking data on long-term safety. Pharmaceutical companies exploited this gap by promoting opioids for chronic pain, a condition for which their efficacy remains unproven. For example, Purdue Pharma funded seemingly independent organizations like the American Pain Society, which published guidelines advocating opioids as a first-line treatment. This industry-driven narrative permeated medical education, leaving doctors ill-equipped to manage pain without opioids. The result? A 2017 study found that 1 in 5 Medicare patients with non-cancer pain received opioids, often at dangerously high dosages exceeding 90 morphine milligram equivalents (MME) per day.
To combat these tactics, practical steps must be taken. First, healthcare providers should scrutinize pharmaceutical marketing materials and rely on unbiased sources for treatment guidelines. Tools like the CDC’s opioid prescribing guidelines offer evidence-based recommendations, such as limiting initial prescriptions to 3–7 days and avoiding dosages above 50 MME per day. Second, policymakers must enforce stricter regulations on drug marketing, including transparency in funding for medical education and research. Finally, patients should be educated about the risks of opioids and empowered to explore alternative pain management strategies, such as physical therapy or non-opioid medications. By dismantling the influence of aggressive marketing, we can begin to reverse the tide of the opioid epidemic.
Tesla Fuel Savings: Myth or Reality? Uncovering the Truth
You may want to see also
Explore related products






![]()
Socioeconomic factors driving substance misuse
The opioid epidemic, a crisis that has ravaged communities across the globe, is not solely driven by individual choices or medical practices. A deeper examination reveals a complex web of socioeconomic factors that create an environment ripe for substance misuse. Poverty, for instance, is a significant predictor of opioid addiction. Individuals living below the poverty line often face limited access to quality healthcare, education, and stable employment, leaving them more vulnerable to the allure of opioids as a means of escape or coping. A study by the Centers for Disease Control and Prevention (CDC) found that counties with higher poverty rates had significantly higher rates of opioid-related deaths, underscoring the inextricable link between economic hardship and substance misuse.
Consider the role of education, or the lack thereof, in perpetuating this cycle. Low literacy rates and inadequate access to quality schooling often correlate with higher unemployment and underemployment. Without stable, well-paying jobs, individuals may turn to opioids as a way to numb the stress and despair of their circumstances. For example, in rural areas where industries like coal mining or manufacturing have declined, leaving behind economic devastation, opioid misuse rates tend to soar. A 2018 report by the National Institute on Drug Abuse (NIDA) highlighted that adults without a high school diploma are twice as likely to misuse prescription opioids compared to college graduates. This disparity is not merely a coincidence but a reflection of systemic inequalities that foster desperation and hopelessness.
Another critical socioeconomic factor is the lack of affordable mental health services. In communities where poverty is pervasive, mental health resources are often scarce or prohibitively expensive. This void leaves individuals struggling with anxiety, depression, or trauma with few healthy coping mechanisms. Opioids, whether prescribed or obtained illicitly, become a readily available alternative. For instance, a person working multiple low-wage jobs to make ends meet may not have the time or financial means to seek therapy, making painkillers a seemingly practical solution to manage both physical and emotional pain. The American Psychological Association notes that untreated mental health issues are a significant risk factor for substance misuse, particularly in low-income populations.
Housing instability further exacerbates the problem. Individuals experiencing homelessness or living in substandard conditions face constant stress and insecurity, which can drive them toward substance use as a form of self-medication. A 2020 study published in the *Journal of Urban Health* found that homeless individuals were 18 times more likely to use opioids than the general population. The lack of a stable living environment not only increases exposure to drugs but also limits access to recovery programs and support systems. Addressing housing instability, therefore, is not just a matter of social welfare but a critical step in combating the opioid epidemic.
To break the cycle of socioeconomic factors fueling substance misuse, targeted interventions are essential. Policymakers must prioritize initiatives that address poverty, improve access to education and mental health services, and provide stable housing. For example, implementing job training programs in economically depressed areas can offer viable alternatives to opioid use. Similarly, expanding Medicaid coverage to include comprehensive mental health and addiction treatment services can make a significant difference. Practical steps like these, while not a panacea, can disrupt the socioeconomic drivers of the opioid epidemic and offer hope to those most at risk. The challenge is immense, but so is the potential for change when systemic issues are confronted head-on.
Does Zoomcar Include Fuel? Understanding Rental Costs and Policies
You may want to see also
Frequently asked questions
Overprescription of opioid pain medications by healthcare providers has been a significant contributor to the opioid epidemic. Excessive prescribing increases access to opioids, leading to misuse, addiction, and diversion of these drugs into illicit markets.
The rise of potent and inexpensive illicit opioids, particularly fentanyl, has exacerbated the opioid epidemic. Fentanyl is often mixed with other drugs, increasing the risk of overdose and death due to its high potency and unpredictability.
Socioeconomic factors such as poverty, lack of access to healthcare, unemployment, and mental health issues play a critical role in fueling the opioid epidemic. These conditions often lead individuals to seek opioids as a coping mechanism.
Limited access to affordable and effective addiction treatment, including medication-assisted treatment (MAT), prevents many individuals from receiving the help they need. This lack of resources perpetuates the cycle of addiction and increases the risk of overdose and other adverse outcomes.