The question of whether oxygen fuels cancer is a complex and often misunderstood topic in oncology. While it is true that cancer cells thrive in low-oxygen environments, a condition known as hypoxia, this does not mean that oxygen directly fuels cancer growth. Instead, hypoxia triggers adaptive mechanisms in cancer cells, such as the activation of hypoxia-inducible factors (HIFs), which promote angiogenesis, metabolic changes, and treatment resistance. Conversely, well-oxygenated tissues can enhance the effectiveness of certain cancer therapies, such as radiation and some chemotherapy drugs, which rely on oxygen to generate reactive oxygen species that damage cancer cells. Thus, the relationship between oxygen and cancer is nuanced, involving both tumor-promoting and tumor-suppressing effects depending on the context.
| Characteristics | Values |
|---|---|
| Oxygen's Role in Cancer Metabolism | Cancer cells often exhibit the Warburg effect, where they prefer glycolysis (fermentation of glucose) even in the presence of oxygen, producing less ATP but supporting rapid growth. However, some cancer cells utilize oxidative phosphorylation (OXPHOS) in well-oxygenated regions, highlighting heterogeneity. |
| Hypoxia and Tumor Aggressiveness | Low oxygen (hypoxia) in tumors promotes aggressiveness by activating HIF-1α, which upregulates genes involved in angiogenesis, metastasis, and treatment resistance. |
| Oxygen and Radiation Therapy | Well-oxygenated cancer cells are more sensitive to radiation therapy due to the formation of DNA-damaging free radicals. Hypoxic cells are more resistant. |
| Oxygen in Chemotherapy | Some chemotherapy drugs (e.g., doxorubicin) require oxygen for optimal cytotoxicity, while hypoxic conditions can reduce their effectiveness. |
| Hyperbaric Oxygen Therapy (HBOT) | HBOT increases oxygen levels in tissues, potentially enhancing the efficacy of radiation therapy and certain chemotherapy drugs, though its role in cancer treatment remains debated and is not universally accepted. |
| Oxygen and Immune Response | Adequate oxygenation supports immune cell function, including T-cell activity, which is crucial for recognizing and attacking cancer cells. Hypoxia can suppress immune responses. |
| Oxygen Paradox | While oxygen is essential for normal cellular function, excessive oxygen (hyperoxia) can generate reactive oxygen species (ROS), potentially causing DNA damage and promoting cancer progression in certain contexts. |
| Current Research Focus | Ongoing studies explore targeting hypoxia-induced pathways (e.g., HIF inhibitors) and combining oxygen-enhancing therapies with traditional treatments to improve outcomes. |
| Conclusion | Oxygen does not directly "fuel" cancer but plays a complex role in tumor biology, influencing metabolism, treatment response, and disease progression. Its effects depend on tumor microenvironment and cellular context. |
Explore related products


$13.67 $15.95

$12.42 $19.95


What You'll Learn
- Oxygen’s role in cellular respiration and cancer cell metabolism differences
- Hypoxia (low oxygen) and its impact on tumor growth and aggression
- Does hyperbaric oxygen therapy (HBOT) inhibit or promote cancer spread?
- Warburg effect: Cancer cells’ reliance on glycolysis even in oxygen presence
- Oxygen’s influence on immune response and cancer cell survival mechanisms
![]()
Oxygen’s role in cellular respiration and cancer cell metabolism differences
Oxygen is the lifeblood of cellular respiration, the process by which cells generate energy in the form of ATP. In normal cells, oxygen acts as the final electron acceptor in the mitochondrial electron transport chain, enabling the efficient breakdown of glucose and other nutrients. This process, known as oxidative phosphorylation, is highly efficient, yielding up to 36 ATP molecules per glucose molecule. However, cancer cells often exhibit a peculiar metabolic shift, favoring glycolysis even in the presence of adequate oxygen—a phenomenon known as the Warburg effect. This inefficiency, producing only 2 ATP per glucose molecule, raises the question: why would cancer cells abandon a more productive energy pathway?
To understand this paradox, consider the unique demands of rapidly proliferating cancer cells. Unlike normal cells, cancer cells prioritize biomass production over energy efficiency. Glycolysis provides intermediate metabolites like ribose and NADPH, which are essential for synthesizing nucleotides, lipids, and proteins—the building blocks of new cells. Oxygen, while critical for energy production in healthy cells, becomes a secondary player in this context. Cancer cells adapt to hypoxic (low-oxygen) environments by upregulating glycolytic enzymes, ensuring their survival and growth even in oxygen-deprived tumor regions. This metabolic reprogramming is not a flaw but a strategic advantage, allowing cancer cells to thrive under conditions that would stifle normal cells.
From a practical standpoint, understanding oxygen’s role in cancer metabolism has significant implications for treatment. For instance, hyperbaric oxygen therapy (HBOT), which involves administering 100% oxygen at increased atmospheric pressure, has been explored as a potential adjunct to cancer therapy. By elevating tissue oxygen levels, HBOT aims to sensitize cancer cells to radiation and certain chemotherapy drugs, which are more effective in oxygen-rich environments. However, caution is warranted: excessive oxygen can also induce oxidative stress, potentially damaging both cancerous and healthy cells. Dosage and timing are critical; HBOT sessions typically range from 60 to 90 minutes, administered 5 days a week for several weeks, under strict medical supervision.
A comparative analysis of oxygen’s role in normal versus cancer cell metabolism reveals a striking divergence in priorities. Normal cells optimize for energy efficiency, leveraging oxygen to maximize ATP production. Cancer cells, in contrast, prioritize growth and survival, exploiting glycolysis to fuel their rapid proliferation. This metabolic flexibility underscores the resilience of cancer cells and highlights the challenge of targeting their energy pathways without harming healthy tissues. For example, drugs like 2-deoxyglucose, which inhibit glycolysis, have shown promise in preclinical studies but must be carefully dosed to avoid systemic toxicity, particularly in metabolically active organs like the brain and muscles.
In conclusion, oxygen’s role in cellular respiration is fundamentally altered in cancer cell metabolism. While it remains essential for energy production in healthy cells, cancer cells rewire their metabolism to thrive in oxygen-limited environments, prioritizing growth over efficiency. This adaptation not only sustains their survival but also presents a therapeutic challenge. By targeting the unique metabolic vulnerabilities of cancer cells, such as their reliance on glycolysis, researchers can develop more precise and effective treatments. Practical strategies like HBOT and glycolysis inhibitors offer promising avenues, but their application requires careful consideration of dosage, timing, and potential side effects. Understanding these differences is key to unlocking new approaches in the fight against cancer.
Understanding Fuel Assistance: How Programs Help Low-Income Families Stay Warm
You may want to see also
Explore related products






![]()
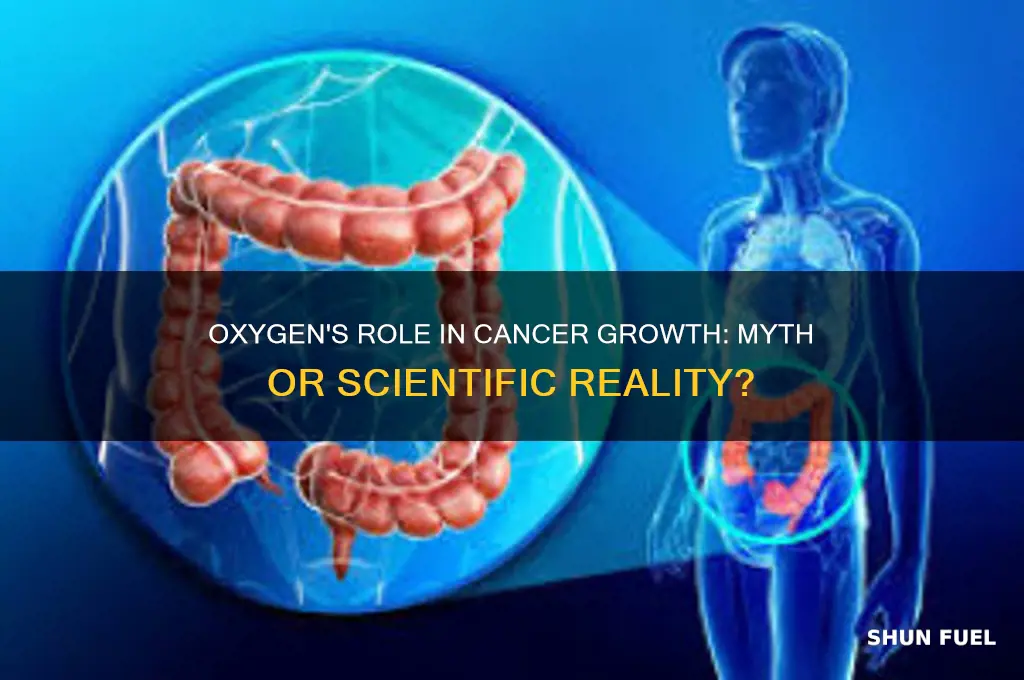
Hypoxia (low oxygen) and its impact on tumor growth and aggression
Tumors thrive in environments where oxygen is scarce, a condition known as hypoxia. This isn’t merely a byproduct of their chaotic growth; it’s a strategic advantage. Hypoxic regions within tumors activate pathways that enhance survival, proliferation, and metastasis. For instance, hypoxia-inducible factor-1 (HIF-1), a protein upregulated in low-oxygen conditions, drives the expression of genes involved in angiogenesis, glucose metabolism, and resistance to apoptosis. This adaptation turns hypoxia into a catalyst for tumor aggression, making it a critical target in cancer research.
Consider the practical implications for treatment. Hypoxic tumors are notoriously resistant to radiation therapy, which relies on oxygen to generate DNA-damaging free radicals. Studies show that hypoxic cells can require up to three times the radiation dose of well-oxygenated cells to achieve the same effect. Chemotherapy is similarly hindered, as many drugs depend on oxygen-dependent pathways to function. Patients with hypoxic tumors often face poorer prognoses, underscoring the need for strategies like hyperbaric oxygen therapy or hypoxia-activated prodrugs to sensitize tumors to treatment.
From a comparative standpoint, hypoxia’s role in cancer mirrors its impact on wound healing, where it initially promotes tissue repair but can lead to chronic inflammation if prolonged. In tumors, this duality is more sinister. While hypoxia triggers angiogenesis to restore oxygen supply, the resulting blood vessels are often dysfunctional, perpetuating a cycle of low oxygen and increased aggression. This contrasts with normal tissues, where hypoxia is transient and tightly regulated. Understanding this distinction could inform therapies that disrupt tumor-specific responses to low oxygen.
For those at risk—particularly individuals over 50 or with pre-existing conditions like chronic obstructive pulmonary disease (COPD)—monitoring tissue oxygenation could be a preventive measure. Wearable devices that track oxygen saturation levels, though not yet standard in cancer prevention, offer a glimpse into future strategies. Pairing these with lifestyle changes, such as regular aerobic exercise to improve oxygen delivery, may reduce the microenvironmental conditions that foster tumor growth. While not a cure, such proactive steps could mitigate hypoxia’s role in cancer progression.
Ultimately, hypoxia’s impact on tumor growth and aggression highlights a paradox: while oxygen is essential for life, its deprivation becomes a weapon in the hands of cancer. Addressing hypoxia requires a multifaceted approach—combining targeted therapies, improved diagnostic tools, and preventive measures. By unraveling the mechanisms through which tumors exploit low oxygen, researchers can develop interventions that strip cancer of this critical advantage, paving the way for more effective treatments.
Fuel Cells: Unlocking Clean Energy Potential and Real-World Efficiency
You may want to see also
Explore related products






![]()
Does hyperbaric oxygen therapy (HBOT) inhibit or promote cancer spread?
Hyperbaric oxygen therapy (HBOT) involves breathing pure oxygen in a pressurized chamber, increasing oxygen levels in the blood and tissues. This treatment is widely used for conditions like decompression sickness and non-healing wounds, but its role in cancer is fiercely debated. Proponents argue that HBOT enhances oxygen delivery to hypoxic tumors, improving the effectiveness of radiation therapy. Critics, however, fear that elevated oxygen levels might stimulate cancer cell growth or angiogenesis, fueling metastasis. This paradox—whether HBOT inhibits or promotes cancer spread—hinges on the dual nature of oxygen in tumor biology.
To understand this duality, consider the Warburg effect, where cancer cells rely on glycolysis even in the presence of oxygen. This inefficiency creates hypoxic regions within tumors, which resist treatment and promote aggressiveness. HBOT, by flooding tissues with oxygen, could theoretically reverse hypoxia, sensitizing cancer cells to radiation or chemotherapy. Clinical studies, such as a 2018 trial in *Radiotherapy and Oncology*, demonstrated improved outcomes in patients with head and neck cancer when HBOT was combined with radiation. However, these benefits are context-dependent; not all cancers respond similarly, and timing is critical. For instance, HBOT administered during the proliferative phase of tumor growth might inadvertently support rapid cell division.
Practical application of HBOT in cancer care requires precision. Sessions typically last 60–90 minutes, with pressures ranging from 2.0 to 2.5 atmospheres absolute (ATA). Protocols vary, but a common regimen involves 20–40 sessions, often alongside radiation or chemotherapy. Patients must avoid petroleum-based products before treatment to prevent fire risk, and those with untreated pneumothorax or certain lung conditions are contraindicated. While HBOT is generally safe, side effects like ear pressure, sinus pain, or temporary nearsightedness can occur. Critically, HBOT should never replace standard cancer treatments but rather complement them under expert supervision.
A comparative analysis of HBOT’s risks and benefits reveals a nuanced picture. Animal studies, such as a 2015 experiment in *PLOS One*, showed that HBOT reduced metastasis in breast cancer models by normalizing blood vessels and enhancing drug delivery. Conversely, a 2017 study in *Cancer Research* suggested that excessive oxygen might activate hypoxia-inducible factor-1 (HIF-1), a protein linked to tumor progression. This discrepancy underscores the importance of individualized treatment plans. For example, HBOT may be more beneficial in early-stage cancers or those with confirmed hypoxia, while advanced or highly vascularized tumors might warrant caution.
In conclusion, HBOT’s impact on cancer spread is not binary but contingent on factors like tumor type, stage, and treatment timing. While it holds promise as an adjuvant therapy, particularly in hypoxic tumors, its potential to promote cancer growth cannot be ignored. Patients and clinicians must weigh these risks against benefits, relying on evidence-based guidelines and ongoing research. As the field evolves, HBOT may emerge as a valuable tool in the oncologist’s arsenal—but only when applied judiciously.
Does Ola Outstation Cover Fuel Costs? A Comprehensive Guide
You may want to see also
Explore related products






![]()
Warburg effect: Cancer cells’ reliance on glycolysis even in oxygen presence
Cancer cells exhibit a peculiar metabolic behavior known as the Warburg effect, where they favor glycolysis—a less efficient energy pathway—even in the presence of ample oxygen. This contrasts sharply with normal cells, which switch to oxidative phosphorylation (OXPHOS) under aerobic conditions to maximize ATP production. The Warburg effect is not merely a quirk but a critical adaptation that supports the rapid growth and survival of cancer cells. By fermenting glucose to lactate, even when oxygen is available, cancer cells generate ATP quickly and produce intermediates essential for biomass synthesis, such as nucleotides and lipids. This metabolic shift is now recognized as a hallmark of cancer, offering both insights into tumor biology and potential therapeutic targets.
To understand the Warburg effect, consider the following analogy: imagine a factory designed to produce energy efficiently but suddenly retools its machinery to prioritize speed over efficiency. This is akin to cancer cells opting for glycolysis, which yields only 2 ATP molecules per glucose molecule compared to the 36 ATP from OXPHOS. However, this trade-off provides cancer cells with a survival advantage. Glycolysis occurs in the cytoplasm and is faster, enabling cells to meet the high energy demands of uncontrolled proliferation. Additionally, the Warburg effect reduces oxidative stress by minimizing the production of reactive oxygen species (ROS), which are byproducts of mitochondrial respiration and can damage cellular components.
Clinically, the Warburg effect has practical implications for cancer diagnosis and treatment. Positron emission tomography (PET) scans exploit this phenomenon by using fluorodeoxyglucose (FDG), a radioactive glucose analog, to highlight areas of high glucose uptake, indicative of cancerous tissue. Therapeutically, targeting glycolysis has emerged as a promising strategy. Drugs like 2-deoxyglucose (2-DG), which inhibits glycolysis, are being investigated in clinical trials. However, caution is warranted, as inhibiting glycolysis alone may not be sufficient; cancer cells can adapt by upregulating alternative pathways, such as glutamine metabolism. Combining glycolytic inhibitors with other therapies, like chemotherapy or immunotherapy, may enhance efficacy.
A critical takeaway from the Warburg effect is its role in the tumor microenvironment. As cancer cells consume glucose voraciously, they deplete nutrients in their surroundings, creating a hostile environment for immune cells and normal tissues. This metabolic competition can suppress immune responses, contributing to tumor progression. Strategies to modulate the tumor microenvironment, such as enhancing nutrient availability for immune cells or inhibiting lactate production, could complement traditional cancer treatments. For instance, dietary interventions like calorie restriction or ketogenic diets, which reduce glucose availability, are being explored as adjunctive therapies to starve cancer cells of their primary fuel source.
In summary, the Warburg effect is not just a metabolic anomaly but a strategic adaptation that fuels cancer’s aggressive behavior. By understanding its mechanisms and implications, researchers and clinicians can develop targeted interventions that disrupt cancer’s energy supply chain. From diagnostic tools like PET scans to therapeutic strategies combining metabolic inhibitors with immunotherapy, the Warburg effect offers a lens through which to view cancer as a disease of dysregulated metabolism. Practical steps, such as monitoring glucose intake and exploring metabolic therapies, could empower patients and clinicians alike in the fight against cancer.
Understanding Fuel Meters: How They Measure and Monitor Fuel Consumption
You may want to see also
Explore related products


![Sparthos High Altitude Mask - Simulate High Altitudes - for Gym, Cardio, Fitness, Running, Endurance and HIIT Training [16 Breathing Levels]](https://m.media-amazon.com/images/I/6166Hn2BcSL._AC_UY218_.jpg)



![]()
Oxygen’s influence on immune response and cancer cell survival mechanisms
Oxygen's role in the body is a double-edged sword, particularly when it comes to cancer. While it is essential for the survival of healthy cells, its influence on immune response and cancer cell survival mechanisms is complex and multifaceted. On one hand, oxygen is a critical component in the functioning of immune cells, such as T-lymphocytes and natural killer cells, which rely on aerobic metabolism to mount effective responses against cancer cells. For instance, a study published in *Nature Immunology* highlights that oxygen availability can enhance the cytotoxic activity of CD8+ T cells, making them more efficient in targeting and eliminating cancer cells. However, this same oxygen can also promote the survival of cancer cells through mechanisms like angiogenesis and metabolic adaptation, creating a paradoxical relationship that challenges treatment strategies.
Consider the Warburg effect, a phenomenon where cancer cells preferentially use glycolysis for energy production even in the presence of oxygen, a process known as aerobic glycolysis. This metabolic shift allows cancer cells to survive in hypoxic (low-oxygen) environments, which are common in rapidly growing tumors. Paradoxically, increasing oxygen levels in tumors through hyperbaric oxygen therapy (HBOT) has been explored as a potential treatment. HBOT involves administering 100% oxygen at pressures greater than 1 atmosphere, aiming to increase oxygen delivery to tissues. While some preclinical studies suggest HBOT can enhance the efficacy of radiation therapy by re-oxygenating hypoxic tumor cells, making them more susceptible to treatment, clinical results have been mixed. For example, a 2020 review in *Cancer Treatment Reviews* notes that HBOT’s effectiveness depends on factors like tumor type, stage, and individual patient response, underscoring the need for personalized approaches.
The immune system’s response to oxygen is equally nuanced. Hypoxia in tumors can suppress immune function by inhibiting the activity of immune cells and promoting the recruitment of immunosuppressive cells like regulatory T cells (Tregs). Conversely, adequate oxygenation can activate immune checkpoints and enhance the presentation of tumor antigens, thereby boosting anti-tumor immunity. Immunotherapies, such as checkpoint inhibitors, often work better in well-oxygenated tumors, as oxygen supports the infiltration and function of immune cells. For patients undergoing immunotherapy, maintaining optimal oxygen levels through interventions like supplemental oxygen (2–4 L/min via nasal cannula) or lifestyle modifications (e.g., regular aerobic exercise) may improve outcomes. However, excessive oxygen can also induce oxidative stress, potentially damaging healthy cells and creating a pro-inflammatory environment that could inadvertently support cancer progression.
Practical considerations for managing oxygen’s influence on cancer involve balancing its benefits and risks. For instance, patients with advanced cancers or those undergoing radiation therapy may benefit from controlled oxygen therapy to enhance treatment efficacy. However, this must be carefully monitored to avoid exacerbating oxidative stress or promoting angiogenesis. Dietary interventions, such as consuming antioxidants (e.g., vitamin C, E, and selenium) in moderation, can help mitigate oxidative damage without compromising the anti-cancer effects of oxygen. Additionally, combining oxygen-based therapies with targeted treatments like hypoxia-activated prodrugs (e.g., tirapazamine) could selectively exploit tumor hypoxia while minimizing harm to normal tissues. Ultimately, understanding oxygen’s dual role in immune response and cancer survival is crucial for developing strategies that tip the balance in favor of the patient.
In conclusion, oxygen’s influence on immune response and cancer cell survival mechanisms is a delicate interplay of promotion and suppression. While it empowers immune cells to combat cancer, it also provides cancer cells with adaptive advantages. Clinicians and patients must navigate this complexity by tailoring oxygen-based interventions to individual needs, considering factors like tumor biology, treatment stage, and overall health. By doing so, oxygen can be harnessed as a tool rather than a fuel for cancer, paving the way for more effective and personalized therapies.
Understanding Fuel Value: A Comprehensive Guide to Accurate Determination
You may want to see also
Frequently asked questions
No, oxygen does not fuel cancer growth. Cancer cells can thrive in both oxygen-rich and oxygen-poor environments, but they often adapt to low-oxygen conditions (hypoxia) through a process called the Warburg effect, where they rely on glycolysis for energy.
While oxygen is essential for healthy cells, simply increasing oxygen levels in the body does not kill cancer cells. Cancer cells have mechanisms to survive in high-oxygen environments, and treatments like hyperbaric oxygen therapy are not proven to cure cancer on their own.
Cancer cells do not "hate" oxygen; they are highly adaptable. Some cancer cells can survive in oxygen-rich conditions, while others thrive in low-oxygen environments. Oxygen alone is not a determinant of cancer cell survival.
Yes, low oxygen levels (hypoxia) in tumors can contribute to cancer aggressiveness. Hypoxia triggers genetic changes that promote tumor growth, metastasis, and resistance to treatments like chemotherapy and radiation.
There is no evidence that breathing more oxygen prevents cancer. Cancer development is influenced by genetic, environmental, and lifestyle factors, not by the amount of oxygen inhaled. Focus on proven prevention strategies like a healthy diet, exercise, and avoiding carcinogens.