Recent research has sparked intriguing questions about the adaptability of breast cancer cells in their quest for survival. One emerging area of interest is the potential for certain breast cancers to switch fuel sources, specifically from estrogen to androgen, as a mechanism to evade treatment and sustain growth. Traditionally, hormone receptor-positive breast cancers have been targeted with therapies that block estrogen signaling. However, emerging evidence suggests that some tumors may develop resistance by leveraging androgen receptors, which could provide an alternative pathway for proliferation. This shift not only challenges current treatment paradigms but also highlights the complexity and resilience of cancer cells. Understanding this phenomenon could pave the way for novel therapeutic strategies to combat hormone-driven breast cancers more effectively.
Explore related products





What You'll Learn
![]()
Androgen receptor expression in breast cancer cells
The role of androgen receptors (ARs) in breast cancer has gained significant attention, particularly in the context of whether breast cancer cells can switch to using androgens as a fuel source. Androgen receptor expression in breast cancer cells is a critical area of study, as it may influence tumor growth, treatment response, and patient outcomes. Traditionally, breast cancer has been categorized based on hormone receptor status, such as estrogen receptor (ER) and progesterone receptor (PR) positivity. However, emerging evidence suggests that ARs, typically associated with prostate cancer, also play a pivotal role in a subset of breast cancers, especially in ER-positive tumors. This finding raises the question of whether breast cancer cells can adapt to utilize androgens as an alternative hormonal driver when estrogen signaling is inhibited.
Androgen receptor expression is detected in approximately 70-80% of ER-positive breast cancers, indicating a potential overlap in hormonal pathways. In these cases, AR signaling may compensate for the loss of estrogen-driven growth, particularly in patients treated with anti-estrogen therapies like aromatase inhibitors or tamoxifen. Preclinical studies have demonstrated that AR activation can promote cell proliferation, survival, and resistance to endocrine therapies in breast cancer cells. This suggests that AR expression may serve as a bypass mechanism, allowing cancer cells to switch to androgen-dependent growth when estrogen signaling is blocked. The crosstalk between estrogen and androgen pathways further complicates this dynamic, as androgens can be locally converted to estrogens within the tumor microenvironment, sustaining ER signaling indirectly.
The clinical implications of AR expression in breast cancer are profound. Patients with AR-positive, ER-positive breast cancer may experience poorer outcomes, particularly in the metastatic setting, due to the potential for AR-mediated resistance to endocrine therapy. This has spurred interest in targeting ARs as a therapeutic strategy in breast cancer. Anti-androgens, such as bicalutamide and enzalutamide, are being investigated in clinical trials to determine their efficacy in AR-positive breast cancer, either as monotherapy or in combination with existing treatments. Early results suggest that AR inhibition could be a viable approach to overcome resistance and improve outcomes in this patient population.
However, the heterogeneity of AR expression and its functional significance in breast cancer remains a challenge. Not all AR-positive breast cancers respond to androgen deprivation, indicating that additional factors, such as AR co-regulators, downstream signaling pathways, and tumor microenvironment, influence AR activity. Furthermore, the role of ARs in ER-negative breast cancer is less clear, though some studies suggest AR signaling may still contribute to tumor progression in these cases. Understanding the molecular mechanisms driving AR expression and its interaction with other hormonal pathways is essential for developing targeted therapies.
In conclusion, androgen receptor expression in breast cancer cells represents a critical mechanism by which tumors may adapt to hormonal therapies and switch to using androgens as a fuel source. This phenomenon is particularly relevant in ER-positive breast cancers, where AR signaling can compensate for estrogen deprivation. Ongoing research aims to elucidate the complex interplay between ARs, ERs, and other pathways to identify novel therapeutic strategies. Targeting ARs in combination with existing treatments holds promise for improving outcomes in patients with AR-positive breast cancer, underscoring the importance of personalized medicine in oncology.
Hydrogen Fuel: The Future of Clean Energy?
You may want to see also
Explore related products






![]()
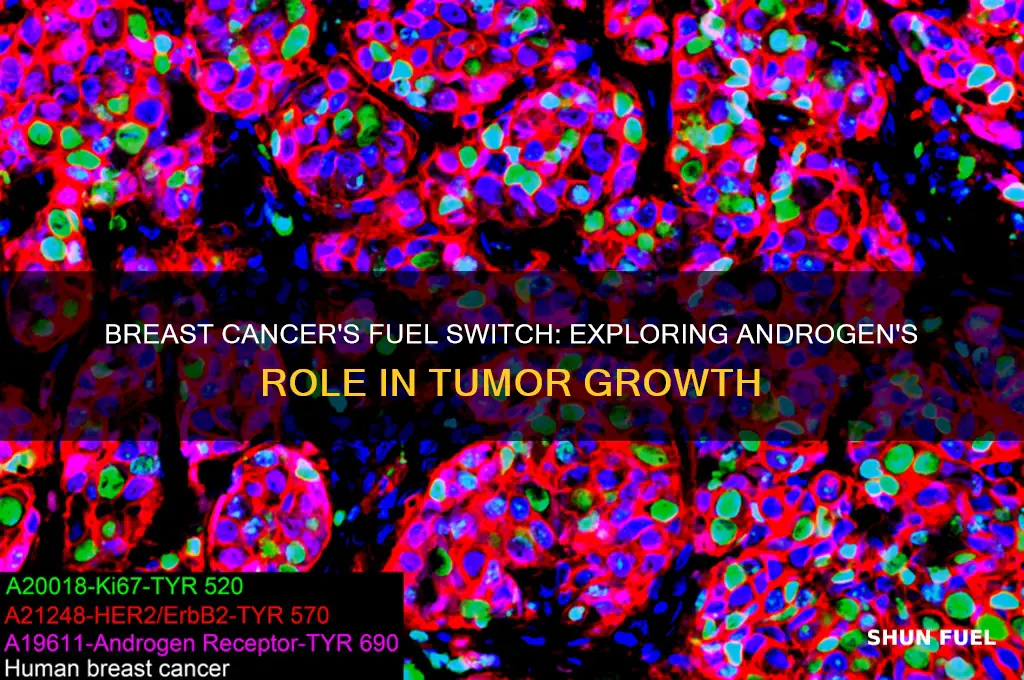
Role of androgen signaling in tumor growth
The role of androgen signaling in tumor growth has gained significant attention, particularly in the context of breast cancer, where the potential for tumors to switch from estrogen-dependent to androgen-fueled growth is a critical area of research. Androgens, traditionally associated with male sexual characteristics, are now recognized as having a complex and multifaceted role in various cancers, including breast cancer. Androgen receptors (ARs) are expressed in a subset of breast cancers, and their activation can promote tumor proliferation, survival, and metastasis. This is particularly relevant in estrogen receptor-positive (ER+) breast cancers that develop resistance to endocrine therapies, such as aromatase inhibitors or tamoxifen, which target estrogen signaling. In these cases, androgen signaling may emerge as an alternative pathway to sustain tumor growth, highlighting the plasticity of cancer cells in adapting to therapeutic pressures.
Androgen signaling in breast cancer is mediated through the AR, which, upon ligand binding, translocates to the nucleus and regulates gene expression. Studies have shown that AR activation can upregulate genes involved in cell cycle progression, anti-apoptotic pathways, and epithelial-mesenchymal transition (EMT), all of which contribute to tumor growth and aggressiveness. Additionally, androgens can cross-talk with other signaling pathways, such as growth factor receptors (e.g., HER2) and the PI3K/AKT/mTOR pathway, further enhancing their oncogenic potential. This cross-talk underscores the complexity of androgen signaling and its ability to integrate with other cellular processes to drive tumor progression.
Emerging evidence suggests that breast cancers, particularly those with low estrogen receptor expression or those resistant to estrogen deprivation therapies, may exploit androgen signaling to fuel their growth. For instance, in ER+/AR+ breast cancers, androgens can compensate for the loss of estrogen-driven proliferation, enabling tumors to bypass the inhibitory effects of anti-estrogen therapies. This phenomenon is supported by clinical observations where AR expression is associated with poorer outcomes in patients treated with endocrine therapies. Furthermore, preclinical models have demonstrated that androgen deprivation or AR inhibition can suppress tumor growth in these contexts, providing a rationale for targeting androgen signaling in breast cancer treatment.
The therapeutic implications of androgen signaling in breast cancer are profound. AR-targeted therapies, such as AR antagonists (e.g., enzalutamide) or androgen synthesis inhibitors, are being investigated as potential treatments for AR+ breast cancers, especially in patients who have progressed on standard endocrine therapies. Combination strategies that simultaneously target estrogen and androgen signaling pathways are also being explored to prevent tumor adaptation and resistance. However, challenges remain, including the heterogeneity of AR expression within tumors and the need for predictive biomarkers to identify patients most likely to benefit from AR-targeted therapies.
In conclusion, androgen signaling plays a significant role in tumor growth, particularly in breast cancers that develop resistance to estrogen-targeted therapies. The ability of cancer cells to switch to androgen-fueled growth highlights the adaptability of tumor biology and the need for comprehensive therapeutic approaches. Understanding the mechanisms underlying androgen signaling and its cross-talk with other pathways is crucial for developing effective strategies to combat breast cancer progression and improve patient outcomes. Further research and clinical trials are essential to fully elucidate the potential of targeting androgen signaling in this complex disease.
Can 'Us' Exist Without 'Them'? Exploring Identity and Interdependence
You may want to see also
Explore related products

$12.97 $13.97





![]()
Hormonal therapy resistance mechanisms in breast cancer
Breast cancer is a heterogeneous disease, and hormonal therapy, particularly targeting estrogen receptors (ERs), has been a cornerstone of treatment for ER-positive (ER+) tumors. However, resistance to hormonal therapies, such as tamoxifen and aromatase inhibitors, remains a significant clinical challenge. Emerging evidence suggests that breast cancer cells can adapt and switch to alternative hormone pathways, including the androgen receptor (AR) pathway, to sustain growth and survival. This phenomenon raises the question: can breast cancer switch to using androgen to fuel its progression? Understanding the mechanisms underlying this switch is crucial for developing strategies to overcome hormonal therapy resistance.
One key mechanism of hormonal therapy resistance involves the upregulation of the AR pathway in ER+ breast cancer cells. Androgens, traditionally associated with male physiology, also play a role in female breast tissue. In the context of estrogen deprivation induced by aromatase inhibitors or tamoxifen, AR signaling can become activated as a compensatory mechanism. Studies have shown that AR expression is elevated in a subset of ER+ breast cancers, particularly in those resistant to estrogen deprivation therapies. The cross-talk between ER and AR pathways allows cancer cells to bypass the inhibitory effects of hormonal therapy, as AR signaling can drive cell proliferation and survival independently of estrogen.
Another resistance mechanism involves genetic and epigenetic alterations that promote AR-mediated growth. For instance, mutations or amplifications in the AR gene itself or in genes regulating AR expression, such as the androgen-synthesizing enzyme AKR1C3, can enhance AR activity. Additionally, epigenetic modifications, including DNA methylation and histone acetylation, can modulate AR expression and sensitivity to androgens. These alterations enable breast cancer cells to exploit the AR pathway, even in the absence of functional ER signaling, thereby fostering resistance to hormonal therapies.
The tumor microenvironment also plays a critical role in facilitating the switch to AR-driven growth. Androgens are locally produced within the breast tissue by stromal cells, and this intratumoral androgen synthesis can sustain AR signaling in cancer cells. Furthermore, interactions between cancer cells and the surrounding stroma, including fibroblasts and immune cells, can enhance AR activity through paracrine signaling. For example, growth factors such as IGF-1 and TGF-β, secreted by stromal cells, can upregulate AR expression and activity, promoting resistance to hormonal therapy.
Clinically, targeting the AR pathway has emerged as a promising strategy to overcome hormonal therapy resistance in breast cancer. Anti-androgens, such as bicalutamide and enzalutamide, are being investigated in combination with traditional hormonal therapies to block both ER and AR signaling. Additionally, inhibitors of androgen synthesis, such as abiraterone, have shown potential in preclinical and early clinical studies. However, the complexity of AR signaling and its interplay with other pathways necessitates a personalized approach, as not all patients with hormonal therapy-resistant breast cancer will benefit from AR-targeted therapies.
In conclusion, the ability of breast cancer to switch to using androgen as a fuel represents a significant mechanism of hormonal therapy resistance. This adaptation involves the upregulation of AR signaling, genetic and epigenetic alterations, and contributions from the tumor microenvironment. Understanding these mechanisms is essential for developing effective therapeutic strategies to combat resistance and improve outcomes for patients with ER+ breast cancer. Further research is needed to identify predictive biomarkers and optimize combination therapies that target both ER and AR pathways.
Hydrogen Fuel Cells: Efficient Energy Storage Solution for a Sustainable Future
You may want to see also
Explore related products






![]()
Androgen-fueled breast cancer subtypes and prevalence
Breast cancer is a heterogeneous disease with diverse molecular subtypes, each driven by distinct biological mechanisms. Among these, the role of androgens in fueling certain breast cancer subtypes has gained significant attention. Androgens, traditionally associated with male sexual characteristics, also play a role in female breast tissue, particularly in the context of androgen receptor (AR) expression. Androgen-fueled breast cancer primarily occurs in subtypes where the tumor cells express AR and utilize androgens for growth and survival. This is particularly evident in triple-negative breast cancer (TNBC) and a subset of estrogen receptor-positive (ER+)/human epidermal growth factor receptor 2-negative (HER2-) breast cancers. Understanding the prevalence and characteristics of these androgen-fueled subtypes is crucial for developing targeted therapies.
Triple-negative breast cancer (TNBC) represents one of the most significant subtypes where androgen signaling plays a role. TNBC lacks expression of ER, progesterone receptor (PR), and HER2, making it resistant to conventional hormone therapies. However, approximately 20-50% of TNBC tumors express AR, and these AR-positive TNBCs are more likely to be driven by androgen signaling. Studies have shown that AR expression in TNBC is associated with a distinct molecular profile, often characterized by luminal-like features despite the absence of ER. The prevalence of AR-positive TNBC varies across populations but is generally observed in 10-30% of all TNBC cases. This subtype tends to have a better prognosis compared to AR-negative TNBC, partly due to its responsiveness to androgen deprivation therapies or AR antagonists.
In addition to TNBC, a subset of ER-positive breast cancers also exhibits AR expression and may rely on androgen signaling, particularly in the context of endocrine resistance. When ER-positive breast cancers become resistant to anti-estrogen therapies like tamoxifen or aromatase inhibitors, they may switch to alternative pathways, including androgen signaling, to sustain growth. This phenomenon is observed in approximately 30-50% of ER-positive breast cancers, where AR co-expression is common. The prevalence of this subtype highlights the importance of considering androgen-targeted therapies in the management of endocrine-resistant breast cancers. Preclinical and clinical studies have demonstrated that AR inhibition, either alone or in combination with other therapies, can be effective in this setting.
The prevalence of androgen-fueled breast cancer subtypes varies across different populations and is influenced by factors such as age, ethnicity, and menopausal status. For instance, postmenopausal women with breast cancer are more likely to have AR-positive tumors compared to premenopausal women. Additionally, African American women have a higher prevalence of AR-positive TNBC, which may contribute to disparities in breast cancer outcomes. Understanding these demographic differences is essential for tailoring treatment strategies and improving outcomes in diverse patient populations.
In conclusion, androgen-fueled breast cancer subtypes represent a significant proportion of breast cancers, particularly within TNBC and ER-positive categories. The prevalence of AR expression in these subtypes underscores the potential of androgen-targeted therapies as a viable treatment option. Ongoing research continues to explore the mechanisms by which breast cancer cells switch to androgen signaling and how this knowledge can be translated into effective clinical interventions. As our understanding of androgen-fueled breast cancer evolves, it holds promise for improving personalized medicine approaches in breast cancer management.
Buying Fuel Oil Direct from the Rack: What You Need to Know
You may want to see also
Explore related products



$19.99 $21.99



![]()
Cross-talk between estrogen and androgen pathways in tumors
The concept of cross-talk between estrogen and androgen pathways in tumors is a critical area of research, particularly in understanding how breast cancer cells adapt to survive and proliferate. Breast cancer is traditionally classified based on hormone receptor status, with estrogen receptor (ER)-positive tumors being the most common. However, emerging evidence suggests that androgen receptor (AR) signaling can play a significant role in breast cancer progression, especially in ER-positive tumors. This cross-talk between estrogen and androgen pathways highlights a complex interplay that may enable tumors to switch fuel sources, potentially contributing to therapeutic resistance.
Estrogen signaling is a well-established driver of breast cancer growth, primarily through the activation of ERα, which regulates genes involved in cell proliferation and survival. Androgen signaling, on the other hand, has been historically understudied in breast cancer but is now recognized as a potential alternative pathway for tumor growth. In ER-positive breast cancers, AR is often co-expressed, and its activation can modulate estrogen-driven pathways. For instance, androgens can induce the expression of ERα, enhancing estrogen-dependent transcription. Conversely, in the absence of estrogen, AR signaling can directly promote cell proliferation, suggesting a compensatory mechanism that allows tumors to thrive under hormone-deprived conditions, such as those induced by anti-estrogen therapies like tamoxifen or aromatase inhibitors.
The molecular mechanisms underlying this cross-talk involve shared co-regulators and downstream targets. Both ER and AR belong to the nuclear receptor superfamily and compete for common co-activators and co-repressors, such as SRC-1 and NCOR. This competition can lead to altered transcriptional programs, favoring tumor growth. Additionally, AR signaling can upregulate the expression of estrogen-responsive genes independently of ER, further blurring the lines between these pathways. Studies have also shown that AR can activate the PI3K/AKT/mTOR pathway, a key driver of cell survival and proliferation, providing another layer of cross-talk that supports tumor progression.
Clinically, the interaction between estrogen and androgen pathways has significant implications for breast cancer treatment. Patients with ER-positive/AR-positive tumors may exhibit resistance to anti-estrogen therapies due to the ability of AR signaling to bypass estrogen blockade. This has led to the exploration of AR inhibitors, such as enzalutamide, as potential therapeutic agents in combination with traditional anti-estrogen treatments. However, the complexity of this cross-talk necessitates a nuanced approach, as complete inhibition of both pathways could lead to unintended consequences, such as increased toxicity or the activation of other compensatory mechanisms.
In conclusion, the cross-talk between estrogen and androgen pathways in tumors represents a dynamic and adaptive mechanism that breast cancer cells exploit for survival and growth. Understanding this interplay is crucial for developing more effective therapeutic strategies, particularly for patients whose tumors rely on both pathways. Future research should focus on identifying specific molecular targets and biomarkers that can predict response to combined ER and AR inhibition, ultimately improving outcomes for breast cancer patients.
Can a Faulty Fuel Pump Cause Unusual Noise in Your Car?
You may want to see also
Frequently asked questions
Some breast cancers, particularly those that are estrogen receptor-positive (ER+) and have developed resistance to estrogen-blocking therapies, may adapt to use androgen as an alternative fuel source. This is more common in postmenopausal women where androgen levels can be relatively higher compared to estrogen.
Androgen can promote the growth of certain breast cancer cells, especially in ER+ tumors, by activating signaling pathways that drive cell proliferation. This is particularly relevant in cancers that have become resistant to anti-estrogen therapies, as they may switch to androgen receptors (AR) for survival.
Treatment for androgen-fueled breast cancer may include androgen receptor (AR) inhibitors, such as enzalutamide or bicalutamide, in combination with existing therapies like aromatase inhibitors or CDK4/6 inhibitors. Personalized treatment plans are often tailored based on the tumor's receptor status and genetic profile.